
Amanda's NICU ED Blogs
Neonatal Seizures
Neonatal Seizures 🧠
Have you cared for a patient in the NICU with seizures? Seizures can occur with many issues we see in the NICU (HIE, Stroke, Sepsis, Electrolyte instability, to name a few).
The neonatal brain is uniquely vulnerable, and when seizures happen, they're usually telling us something significant is going on. Understanding thewhybehind seizures helps you anticipate changes, advocate early, and care for these babies with confidence.
Why Do Neonates Have Seizures?
Seizures are caused by abnormally excessive or synchronous electrical activity in the brain. The immature neonatal brain is structurally and functionally wired to fire easily. This is for a few specific reasons:
The fetal and neonatal brain has the highest density of dendritic spines and synapses at any stage of life, which are necessary to facilitate neurogenesis
Glutamate (the major excitatory neurotransmitter) shows exaggerated activity due to increased expression of certain NMDA receptor subunits
GABA (which normally inhibits firing in adults) can actually act as an excitatory neurotransmitter in neonates
That last point about GABA was surprising to me. Here's why it happens: in the immature brain, a transporter called NKCC1 pumps chloride into neurons, while the mature transporter KCC2 (which pumps chloride out) hasn't fully developed yet. This creates higher-than-normal chloride inside the neuron. So when GABA opens its receptor channel, chloride flows out instead of in. So the neuron depolarizes rather than being inhibited. After birth, KCC2 gradually matures and restores normal GABA-mediated inhibition.
Main takeaway:The neonatal brain is primed to fire easily, especially under stress.
Common Causes of Seizures
The vast majority of neonatal seizures (around 67–80%) are acute symptomatic events, meaning they're provoked by an acute insult to the brain, not epilepsy (which requires unprovoked, recurring seizures).
The most common causes in high-income countries include:
Hypoxic-ischemic encephalopathy (HIE):approximately 40% of all neonatal seizures. The leading cause in term, post-term, and late preterm neonates
Ischemic stroke:roughly 20% of cases
Intracranial hemorrhage (ICH):approximately 10%; more common in our preemies.
Infection:including bacterial meningitis and HSV
Electrolyte abnormalities:hypocalcemia, hypomagnesemia, hyponatremia
Hypoglycemia
Each of these disrupts the delicate ion balance and energy supply the neuron depends on. ATP failure, excessive glutamate release, and electrolyte shifts all lower the seizure threshold and push an already-vulnerable brain over the edge.
Timing matters too.HIE seizures often appear within the first 12–24 hours after birth or during rewarming from therapeutic hypothermia. Stroke- and hemorrhage-related seizures typically present later. Knowing the underlying etiology helps you anticipate when to be watching most closely.
Clinical Presentation
Neonatal seizures are categorized as electroclinical (visible clinical signs + EEG correlate) or electrographic-only (seen on EEG with no visible clinical signs).
When there are clinical signs, you might see:
Lip smacking, chewing, tongue protrusion, or sucking
Eye deviation or nystagmus
Focal clonic movements (rhythmic jerking of a limb)
Bicycling or swimming movements
Apnea or desaturation
Tonic posturing
Keep in mind that more than half of electrographic neonatal seizures have no visible clinical signs at all. In one study from an Irish NICU, only 27% of clinically suspected seizures actually had an EEG correlate while the electrographic seizures that were happening went largely unrecognized (Murray et al., 2008).
So, if more than have the time we can’t visually see the seizures how do we know?
Diagnosing Seizures:
Continuous EEG (cEEG) is the gold standard for diagnosing neonatal seizures.
cEEG is indicated in any neonate with:
Suspected or confirmed HIE
Ischemic or hemorrhagic CNS injury
Suspected CNS infection
Pharmacologic neuromuscular blockade or sedation that limits clinical assessment
Premature neonates with high-grade IVH
Any high-risk neonate where subclinical seizures could go undetected
The American Clinical Neurophysiology Society recommends a minimum of 24 hours of cEEG recording. In neonates undergoing therapeutic hypothermia, monitoring should continue through rewarming, since seizure risk peaks during that window.
Amplitude-integrated EEG (aEEG) can be used when cEEG is unavailable, but it misses short seizures, focal seizures, and seizures spatially distant from its limited electrode placement. It is not recommended for preterm infants, who often have low-amplitude seizures.
Beyond EEG, key diagnostic workup includes:
Bedside and laboratory glucose
Serum electrolytes (calcium, magnesium, sodium)
Blood gas, CBC, blood culture
LP for CSF studies, cultures, and HSV PCR (as soon as the neonate is stable)
Head ultrasound for timely structural evaluation
Brain MRI (preferred imaging modality, including DWI sequences)
Treatment: Treat the Cause First, Then the Seizure
Before reaching for antiseizure medications (ASMs), always ask:Is there a reversible cause that can be corrected?
Seizures caused by hypoglycemia, hypocalcemia, hypomagnesemia, or infection will not respond adequately to ASMs until the underlying cause is addressed.
What treatment should you expect?
Hypoglycemia:IV dextrose 10%, 2 mL/kg bolus, followed by maintenance fluids
Hypocalcemia:calcium gluconate 100 mg/kg IV
Hypomagnesemia:magnesium sulfate 125 mg/kg IV
Infection:empiric broad-spectrum antibiotics and acyclovir without delay, pending cultures
Seizure responsiveness to ASMs also diminishes the longer seizures go on. One study found that neonates treatedwithin 1 hour of seizure onset had significantly lower seizure burden than those treated 2 hours later (Gettings & Soul, 2025).
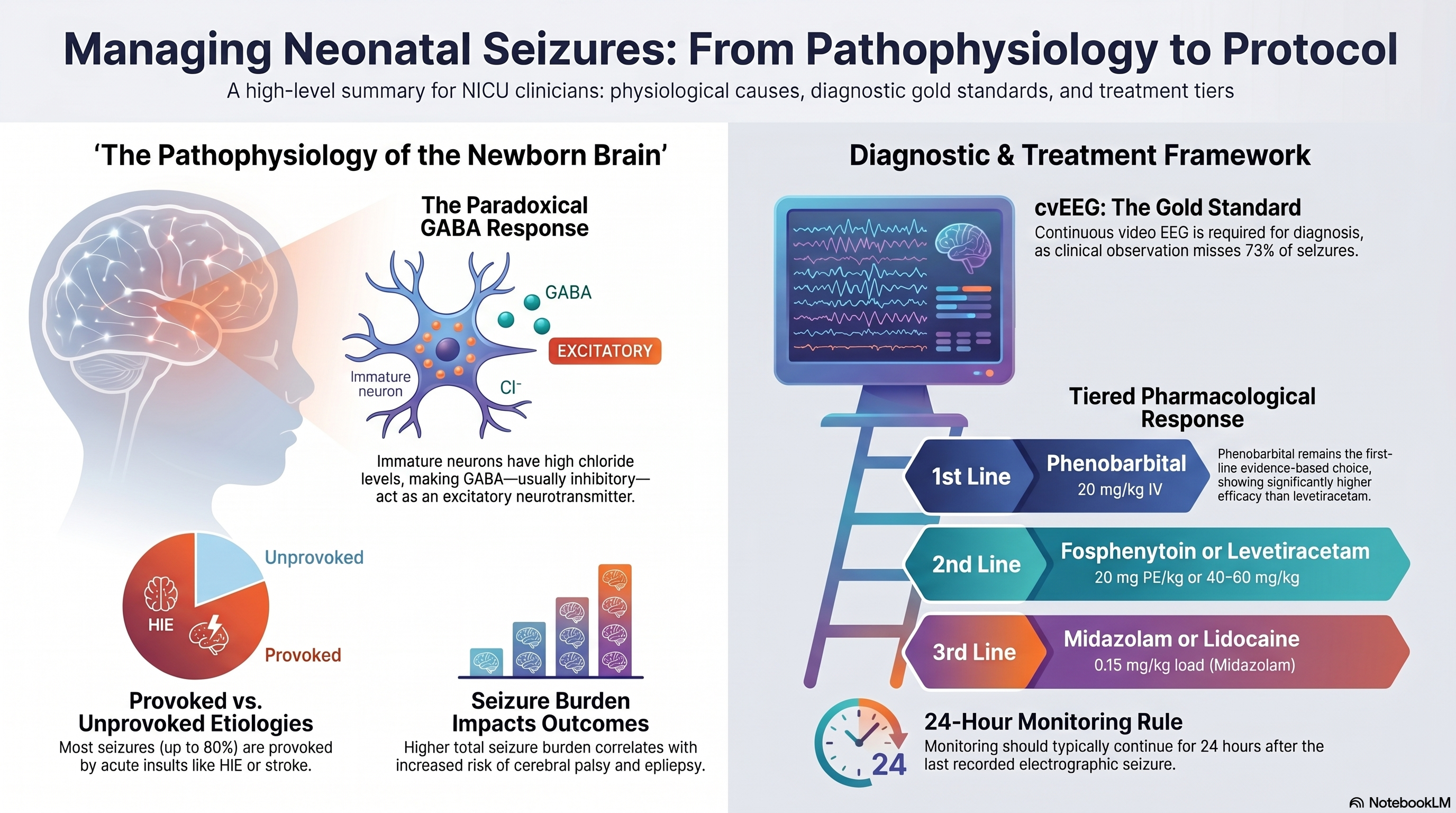
First-Line: Phenobarbital
Phenobarbital remains the only FDA-approved antiseizure medication for neonatal seizures, and it is the established first-line agent.
How it works:Phenobarbital is a GABA agonist that binds to GABA-A receptors, aiming to increase neuronal inhibition.
Efficacy:
40–60% of clinical seizures controlled at standard serum levels (20 mcg/mL)
Up to 70–85% of clinical seizures controlled at higher levels (40 mcg/mL)
In the RCT NEOLEV2 (n = 83), 80% of neonates treated with phenobarbital achieved 24-hour seizure cessation confirmed by cEEG (Sharpe et al., 2020).
Dosing:
Loading dose: 20 mg/kg IV
May repeat in 10–20 mg/kg boluses, targeting serum levels of 40–50 mcg/mL
Maximum cumulative loading dose: 40–50 mg/kg over 24 hours
Maintenance: 4–6 mg/kg/day IV or PO, divided BID or once daily
IV and oral dosing are equivalent (1:1 conversion)
Adverse effects to monitor:Hypotension, respiratory depression, CNS depression, and bradycardia.
Second Line: Fosphenytoin vs Keppra
I don’t know about you but I’ve recently noticed a shift in the second line agent being prescribed in my NeuroNICU. Previously I would see Levetiracetam (Keppra) but lately it’s been Fosphenytoin. Have you seen this where you work? Let’s take a closer look at the two
Fosphenytoin:
Fosphenytoin is a water-soluble prodrug of phenytoin that converts rapidly to phenytoin via plasma esterases. It was developed specifically to avoid the serious administration risks of IV phenytoin. Phenytoin has a pH of 11 and can cause severe hypotension, cardiac arrhythmias, and tissue necrosis ("purple glove syndrome").
How it works: Fosphenytoin blocks voltage-gated sodium channels, stabilizing neuronal membranes and preventing the excessive depolarization that drives seizures. This mechanism is entirely different from phenobarbital's GABA-based action.
The efficacy evidence:A 1999 RCT (Painter et al., n = 59) found phenobarbital and phenytoin equally effective as first-line agents (43% vs. 45% seizure cessation) with combined sequential use reaching 57–62%. As second-line therapy after phenobarbital failure, one prospective multicenter study found phenytoin achieved 56.7% efficacy outperforming levetiracetam (13.8%).
In a 16-center observational cohort study fosphenytoin/phenytoin was found superior to levetiracetam as second-line therapy, with response rates of 45.5% vs. 29% and an adjusted odds ratio of 2.15 (95% CI 1.18–3.9) (Grinspan, 2025). This is a significant finding, and it's driving real practice changes in NICUs and NeuroNICUs (and likely related to the changes I've seen).
Neurodevelopmental effects:A retrospective observational study that transitioned from phenobarbital to fosphenytoin as first-line therapy found comparable acute seizure control between the two, but significantly fewer infants in the fosphenytoin group had moderate-to-severe neurodevelopmental delay at 18–24 months(Alix et al, 2021). This is a hypothesis-generating finding, not definitive evidence, but it's part of why neurologists are paying attention.
A 2021 survey of treatment pathways from 11 large US academic NICUs found that pathways were divided. Fosphenytoin and levetiracetam were equally common as the designated second-line ASM, with no consensus across centers (Keene et al., 2021). More recently, Children's Hospital of Philadelphia updated their NeuroNICU pathway (revised February 2025) to place fosphenytoin explicitly as second-line, with levetiracetam moved to third (CHOP Clinical Pathway, 2025).
Dosing:
Loading dose: 20 mg PE/kg IV (PE = phenytoin equivalents)
Additional doses of 5 mg PE/kg as needed
Maintenance: 6–8 mg PE/kg/day divided every 8 hours
Monitor free phenytoin levels (target 1–2 mcg/mL) or total phenytoin (target 8–15 mcg/mL)
Fosphenytoin has a narrow therapeutic index and requires diligent monitoring
Critical safety considerations:
Cardiac arrhythmias, hypotension, and CNS depression are known adverse effects
Never use fosphenytoin and lidocaine together. They share sodium channel blockade and have additive cardiotoxic risk
Despite its superior safety profile compared to IV phenytoin, fosphenytoin still requires careful line patency monitoring, as extravasation can occur
Poor oral bioavailability means maintenance phenytoin is generally not continued long-term
Levetiracetam:
Levetiracetam is a frequently used second-line option and in specific patient populations, it may actually be the better choice.
How it works:Levetiracetam binds to synaptic vesicle protein SV2A, modulating neurotransmitter release. This is distinct from both phenobarbital and fosphenytoin.
The NEOLEV2 RCT showed levetiracetam at 28% seizure cessation as first-line vs. 80% for phenobarbital. As second-line, a prospective multicenter study found it effective in only 13.8% of cases. The 2026 Moawad meta-analysis (26 studies, 9,854 neonates) found comparable overall efficacy to phenobarbital when both were used as first-line but as second-line specifically, the emerging data favor fosphenytoin.
Safety:Levetiracetam wins when it comes to the safety profile. Moawad et al. (2026) found that phenobarbital carried significantly higher risks of hypotension and respiratory depression compared to levetiracetam. Fosphenytoin carries its own cardiac and hemodynamic risks. For unstable neonates, levetiracetam's side effect profile make it preferable.
When levetiracetam remains preferred:The ILAE 2023 guidelines specifically recommend levetiracetam as the preferred second-line ASM in neonates with cardiac disorders. The arrhythmia risk of fosphenytoin and lidocaine makes them less suitable in neonates with significant hemodynamic instability or hepatic dysfunction.
Dosing:
Loading dose: 40–60 mg/kg IV
Maintenance: 40–60 mg/kg/day IV or PO divided BID
No therapeutic drug monitoring required; 1:1 IV to oral conversion
What does that mean for you at the bedside?
We may start seeing a shift in practice at many NeuroNICUs, especially for the typical patient with HIE or stroke who doesn't have cardiac contraindications.
The ILAE could not reach consensus on a single preferred second-line agent, and the evidence level for this recommendation remains very low.
What this means is:
Fosphenytoin is increasingly favored as second-line for most neonates, particularly where cardiac function is stable and seizure control efficacy is the priority
Levetiracetam remains preferred when hemodynamic or respiratory instability is present, or in neonates with cardiac disease
Your unit's protocol matters: practice varies significantly across institutions, and understanding why your team makes the choices they do helps you participate meaningfully in care
Other Options for Refractory Seizures
When first- and second-line agents fail, there are other options including:
Midazolam— A GABA agonist used as third-line therapy. Significant side effects include hypotension and respiratory depression that will nearly always require mechanical ventilation at the doses needed for refractory seizures.
Lidocaine— Sodium channel blockade, used widely in Europe as second-line after phenobarbital. Good to intermediate efficacy reported in retrospective studies. Do not use after fosphenytoin/phenytoin due to compounding cardiac risk. Requires dose adjustment in neonates <2.5 kg and those on therapeutic hypothermia.
Vitamin-responsive epilepsies— If seizures are refractory to multiple ASMs with no clear acute provoked etiology, empiric trials of pyridoxine, pyridoxal-5-phosphate, and folinic acid should be considered under cEEG monitoring.
When Do We Stop Treatment?
For neonates with acute provoked seizures, seizures typically resolve within 72–96 hours as the underlying cause is treated. Current ILAE guidelines recommend discontinuing ASMs prior to hospital discharge in these neonates (regardless of MRI or EEG findings) because prolonged phenobarbital exposure carries neurodevelopmental risks, and no ASM has been shown to prevent post-neonatal epilepsy. A comparative study found no difference in neurodevelopmental outcomes or epilepsy risk at 2 years between those maintained on ASMs versus those discontinued before discharge (Glass et al., 2021).
Neonates with neonatal-onset epilepsy syndromes (KCNQ2, SCN2A, structural/genetic causes) are a different population entirely and require ongoing ASMs determined by their specific diagnosis.
Prognosis:
Neonatal seizures carry significant morbidity and mortality, but outcome is driven by the underlying cause and seizure burden than by the seizures themselves.
Mortality: approximately 15% in term infants, 35% in preterm infants
Nearly 1 in 3 survivors develop long-term neurologic impairment, including cerebral palsy, epilepsy, or developmental delay
Multiple observational studies and two small RCTs demonstrate that higher seizure burden correlates with worse neurodevelopmental outcomes, greater MRI injury, and increased mortality independent of underlying etiology. This highlights why early recognition and treatment matter.
Takeaways
When something feels "off”... subtle behavior changes, brief apnea, unusual eye movements, a vague sense that this baby is not quite right:
Trust that clinical instinct
Check glucose and labs early
Escalate to the team promptly
Document it precisely (timing, duration, what you observed)
Advocate for EEG monitoring
And when your team is debating fosphenytoin versus levetiracetam — now you understand why that conversation is happening
Cooling Courses from Synapse Care, get 10% off with my code Amanda10

What questions do you have about seizures? Email me back and let me know what you'd like me to cover or if you have any questions.
Wishing you the best
Amanda
Missed my other newsletters? Click here to read them!
Let's Study Together! Join my Certification Course
References
Alix, V., James, M., Jackson, A. H., Visintainer, P. F., & Singh, R. (2021). Efficacy of Fosphenytoin as First-Line Antiseizure Medication for Neonatal Seizures Compared to Phenobarbital.Journal of child neurology,36(1), 30–37.
Children's Hospital of Philadelphia. (2025, February).Neonatal seizure/status epilepticus clinical pathway — N/IICU.https://www.chop.edu/clinical-pathway/neonatal-seizure-status-epilepticus-clinical-pathway
Gettings, J. V., & Soul, J. S. (2025). Updates in neonatal seizures.Clinics in Perinatology, 52, 375–393.https://doi.org/10.1016/j.clp.2025.02.008
Glass, H. C., Soul, J. S., Chang, T., Wusthoff, C. J., Chu, C. J., Massey, S. L., Abend, N. S., Lemmon, M., Thomas, C., Numis, A. L., Guillet, R., Sturza, J., McNamara, N. A., Rogers, E. E., Franck, L. S., McCulloch, C. E., & Shellhaas, R. A. (2021). Safety of Early Discontinuation of Antiseizure Medication After Acute Symptomatic Neonatal Seizures.JAMA neurology,78(7), 817–825.https://doi.org/10.1001/jamaneurol.2021.1437
Grinspan, Z., Singhal, N., Axeen, E., Bhalla, S., Coryell, J., Eschbach, K., Hussain, S. A., Sandoval Karamian, A., Massey, S., Mbwana, J., Morgan, L., Patel, A., Perry, M. S., Romanowski, E., Sands, T., Soul, J., Triplett, R., Wu, J., Yozawitz, E., … Shellhaas, R. (2025, December 6).Phenytoin/fosphenytoin is superior to levetiracetam as second-line therapy for neonatal seizures: An observational cohort study at 16 centers[Conference abstract]. American Epilepsy Society Annual Meeting.https://aesnet.org/abstractslisting/phenytoin-fosphenytoin-is-superior-to-levetiracetam-as-second-line-therapy-for-neonatal-seizures-an-observational-cohort-study-at-16-centers
Guider, A. J., & McPherson, C. (n.d.). Neonatal seizures. InNeonatal CNS disorders(Chapter 12, pp. 225–240). Springer Publishing.
Keene, J. C., Morgan, L. A., Abend, N. S., Amengual-Gual, M., Anderson, A., Arndt, D., Bhalla, S., Chu, C. J., Coryell, J., Gould, A., Guerriero, R. M., Hussain, S. A., Massey, S. L., McBain, K., Parsons, L. C., Pearce, S., Piantino, J., Pryor, S., Rau, S., … Shellhaas, R. A. (2021). Treatment of neonatal seizures: Comparison of treatment pathways from 11 neonatal intensive care units.Pediatric Neurology.https://doi.org/10.1016/j.pediatrneurol.2021.10.004
Moawad, M. H. E., Elettreby, A. M., Alkhawaldeh, I. M., Abdul-Hafez, H. A., Mohammad Ali, A. M. A., Helal, O. M., Karawya, M., AlHusan, A., Allahham, M., Chair, Y., Al Kabi, H. A., Serag, I., & Abouzid, M. (2026). Levetiracetam versus phenobarbital as first-line therapy for neonatal seizures: A comprehensive systematic review and meta-analysis with meta-regression of 26 studies involving 9,854 neonates.BMC Pediatrics, 26, 222.https://doi.org/10.1186/s12887-026-06539-6
Murray DM, Boylan GB, Ali I, et al. (2008). Defining the gap between electrographic seizure burden, clinical expression and staff recognition of neonatal seizures. Arch Dis Child Fetal Neonatal Ed 93(3):F187–91.
Pressler, R. M., Abend, N. S., Auvin, S., Boylan, G., Brigo, F., Cilio, R., Falsaperla, R., Hahn, C. D., Inder, T. E., Jette, N., Kanner, A. M., Kaplan, P. W., Lemmers, P., Nabbout, R., Rakhmaeva, L., Ramantani, G., Ramos-Lizana, J., Rennie, J., Shellhaas, R. A., … Wilmshurst, J. M. (2023). Treatment of seizures in the neonate: Guidelines and consensus-based recommendations — Special report from the ILAE task force on neonatal seizures.Epilepsia, 64(10), 2550–2570.https://doi.org/10.1111/epi.17745
Zeller, B., & Giebe, J. (2015). Pharmacologic management of neonatal seizures.Neonatal Network, 34(4), 239–244.https://doi.org/10.1891/0730-0832.34.4.239


Subscribe to my Mailing List
Get simple explanations of complex NICU topics, certification study tips, and practical bedside insights delivered straight to your inbox.
hey nurses don't miss out
© Copyright 2024. AmandasNICUEd. All rights reserved. | Terms & Conditions | Privacy Policy Contact: [email protected]