
Amanda's NICU ED Blogs
Glucose Homeostasis
Glucose Homeostasis in the NICU:
Why Some Babies Struggle and Others Don't
You're at the bedside. The glucose comes back low. Your brain immediately goes to: feed, supplement, escalate the GIR. But before you act… do you know WHY that number is low? Because the why changes everything….
To answer that question, you need to understand what's actually happening inside that baby's body from the moment the cord is cut.
The Biggest Metabolic Transition After Birth
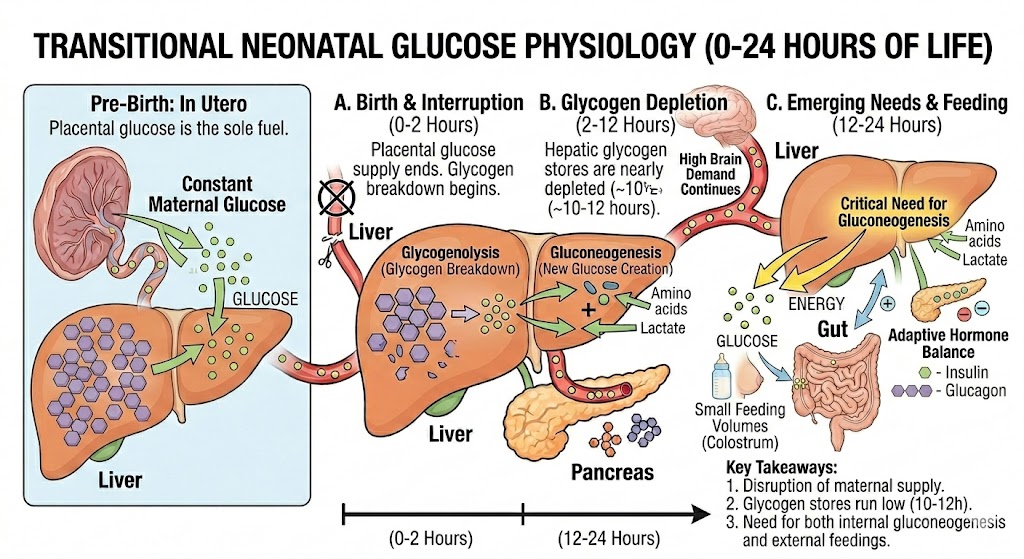
Before birth, the fetus receives a constant supply of glucose from the placenta.
There are no fasting periods, no missed meal or a need for the fetus to make significant amounts of its own glucose. The placenta does all the work.
At delivery, that glucose supply is suddenly interrupted when the umbilical cord is clamped. Within seconds, the newborn must transition from receiving glucose continuously to producing and regulating glucose independently.
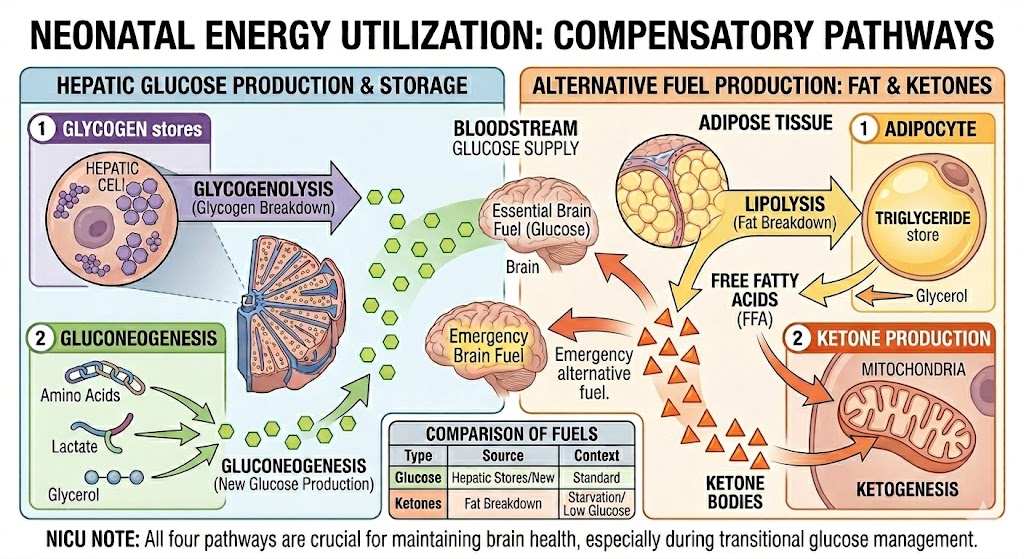
To accomplish this, the body activates several important mechanisms:
Glycogen breakdown (glycogenolysis)
New glucose production (gluconeogenesis)
Fat breakdown (lipolysis)
Ketone production as an alternative fuel source
Glycogen stores in the liver drop from about 50 mg/g at birth to less than 10 mg/g within the first 24 hours of life. The liver is essentially draining its emergency fuel reserve in real time. And gluconeogenesis isn't fully operational until 8 to 12 hours after birth.
That means for those first several hours, a newborn is running on a fuel tank that's actively being depleted, with the backup system not yet fully ready.
For most healthy term infants, the body manages this gap without missing a beat. But when anything disrupts the balance (prematurity, stress, excess insulin, metabolic disease) that narrow window of vulnerability becomes a clinical problem.
Quick question:
Two babies both have a glucose of 40 mg/dL.
Baby A is an Infant of a Diabetic Mother (IDM).
Baby B is a healthy term infant 90 minutes after birth.
Which baby is at greater neurologic risk and why?
The answer comes down to ketones. Keep reading…
But Wait, Even Healthy Babies Drop Their Glucose?
Here's something that surprises a lot of nurses when they first learn it: a transient glucose dip in the first hours of life is completely normal, even expected.
Healthy term, appropriate-for-gestational-age infants routinely have glucose values in the 50s to low 60s mg/dL in the first day of life. If you define normal as within two standard deviations of the mean, the lower limit in the first few hours of life can be as low as the high 30s to low 40s mg/dL.
This phenomenon (transitional neonatal hypoglycemia) is actually driven by a temporary state of relative hyperinsulinism. Insulin doesn't shut off immediately after birth. Ketogenesis is also suppressed during this window, which is why these early dips look different from pathologic hypoglycemia.
What matters most is that it's transient. In healthy infants, glucose stabilizes and rises over the first 48 to 72 hours as glucagon climbs and the counter-regulatory system matures.
The clinical challenge is distinguishing transitional hypoglycemia from hypoglycemia that signals something pathologic. That distinction is where your nursing assessment really matters.
Why Are Newborns So Vulnerable to Hypoglycemia?
Once we get past the normal transitional period, glucose balance comes down to a simple equation:
Glucose Supply = Glucose Utilization
When utilization exceeds supply, blood glucose levels fall.
This can happen for several reasons.
1. Too Much Insulin
Insulin lowers blood glucose by moving glucose from the bloodstream into cells. When insulin levels remain elevated after birth, glucose levels can drop rapidly.
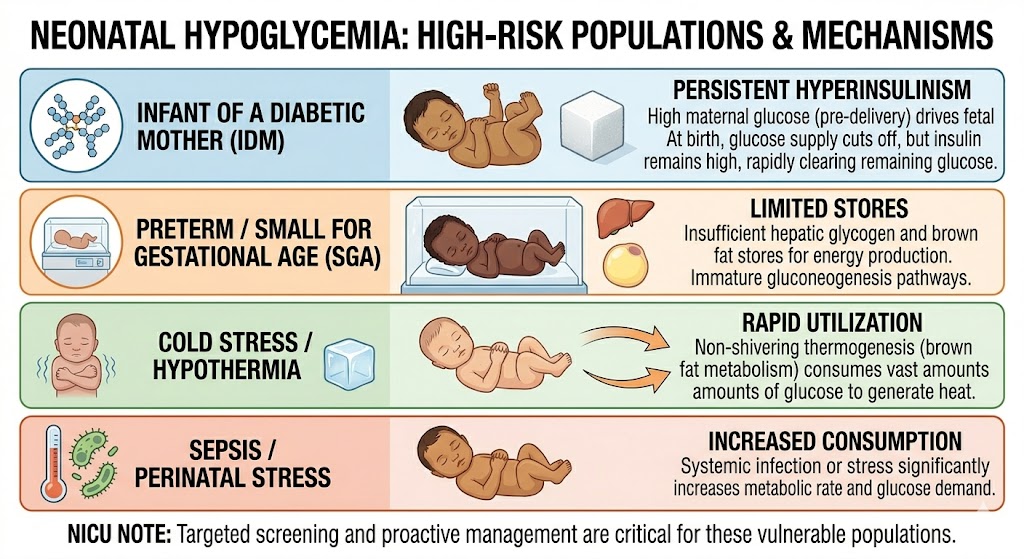
This is the classic mechanism seen in infants of diabetic mothers (IDMs).
During pregnancy, maternal hyperglycemia crosses the placenta and exposes the fetus to high glucose concentrations. In response, the fetal pancreas produces larger amounts of insulin. After birth, maternal glucose delivery stops but insulin levels stay elevated, sometimes for days. This results in a newborn who continues pulling glucose out of the bloodstream despite no longer receiving the maternal glucose supply.
Most IDMs will hit their glucose nadir in the first one to two hours after birth, then gradually stabilize. Knowing that timing helps you anticipate what may happen and prevent injury.
With this in mind, we also need to consider ketones. Under normal circumstances, when glucose drops, the liver ramps up ketone production. Beta-hydroxybutyrate crosses the blood-brain barrier and serves as an alternative fuel for the brain, buying time while glucose recovers.
But in hyperinsulinemic states, insulin suppresses lipolysis and ketogenesis simultaneously. Meaning the brain is not getting glucose OR the backup, ketones. That's why hyperinsulinemic hypoglycemia is particularly dangerous, and why these babies can be neurologically vulnerable even at glucose values that might seem borderline in another context.
Now go back to that question. Baby A is at greater neurologic risk, not just because of the low glucose, but because hyperinsulinism has shut down the ketone backup system entirely. Baby B's transitional dip, by contrast, is part of a normal adaptive process.
2. Not Enough Stored Glycogen
Healthy term infants accumulate glycogen stores during the third trimester. Fetal weight doubles from about 1,700 grams at 32 weeks to roughly 3,400 grams at term. A significant portion of that increase in weight is hepatic glycogen and adipose tissue. These are the metabolic reserves that exist precisely for those first critical hours after birth.
Premature infants miss a major part of this process and small-for-gestational-age infants often have limited glycogen and fat stores as well.
These babies have less metabolic reserve available when the placental glucose supply ends. So when they are born they have very little reserve to sustain their glucose. These are the babies who may look fine in the delivery room and be hypoglycemic by the first glucose check.
3. Increased Glucose Consumption
Some babies use glucose faster than they can produce it.
Common examples include:
Sepsis
Respiratory distress
Hypothermia
Perinatal stress and Asphyxia
Significant cardiac disease
Think of these babies as running their metabolism at a much higher speed. Even normal glucose production may not keep up with demand.
4. Inability to Produce Glucose
Certain endocrine and metabolic disorders impair the body's ability to maintain glucose concentrations.
Examples include:
Congenital hyperinsulinism
Hypopituitarism
Adrenal insufficiency
Growth hormone deficiency
Inborn errors of metabolism
These conditions often present with persistent or recurrent hypoglycemia despite appropriate interventions. If a baby continues to have hypoglycemia despite adequate glucose delivery and feeding, that's the signal to stop troubleshooting the basics and start asking bigger questions.
Why Premature Infants Are Especially Challenging
Premature infants face a perfect storm.
They often have:
Reduced glycogen stores
Limited fat stores
Immature enzyme systems for both glycogenolysis and gluconeogenesis
Increased metabolic demands
Frequent illness or stress
Preterm infants can have markedly reduced glucose-6-phosphatase activity compared to term infants. Glucose-6-phosphatase is the enzyme needed to release glucose from storage. This immaturity can persist for months after birth.
At the same time, the brain remains highly dependent on glucose as its primary energy source. The neonatal brain is proportionally larger (with higher metabolic demand) than an adult brain, requiring two to three times more hepatic glucose production per kilogram of body weight.This combination explains why glucose monitoring is such an important part of NICU care.
Glucose monitoring matters in both directions because hyperglycemia in the NICU is just as physiologically complex as hypoglycemia, and just as easy to misunderstand.
When the Glucose Doesn't Respond: Understanding the Critical Labs
You've escalated. You've increased the GIR. You've fed the baby. And the glucose still isn't responding the way it should.
This is the moment the endocrinologist gets called and critical labs are ordered.
You've heard the words. But do you understand why those labs are being ordered? The answer is simpler than you might think.
These labs will help answer the question: Is this baby mounting an appropriate response to hypoglycemia?
When glucose falls, the body should be in full emergency mode. The critical labs are a snapshot of whether that emergency response is actually happening. If not, which part of the system failed.
When should a critical sample be obtained?
Timing matters enormously. Critical labs must be drawn at the time of hypoglycemia, before correction with dextrose, because the entire interpretation depends on capturing the baby's uncorrected metabolic state. A sample drawn after treatment tells you very little.
In general, a critical sample is indicated when:
Hypoglycemia persists beyond 48 to 72 hours of life
Glucose cannot be maintained above 50 mg/dL in the first 48 hours, or above 60 mg/dL after 48 hours
Hypoglycemia is severe, recurrent, or requires a high glucose infusion rate
The baby has seizures or other neurologic signs associated with low glucose
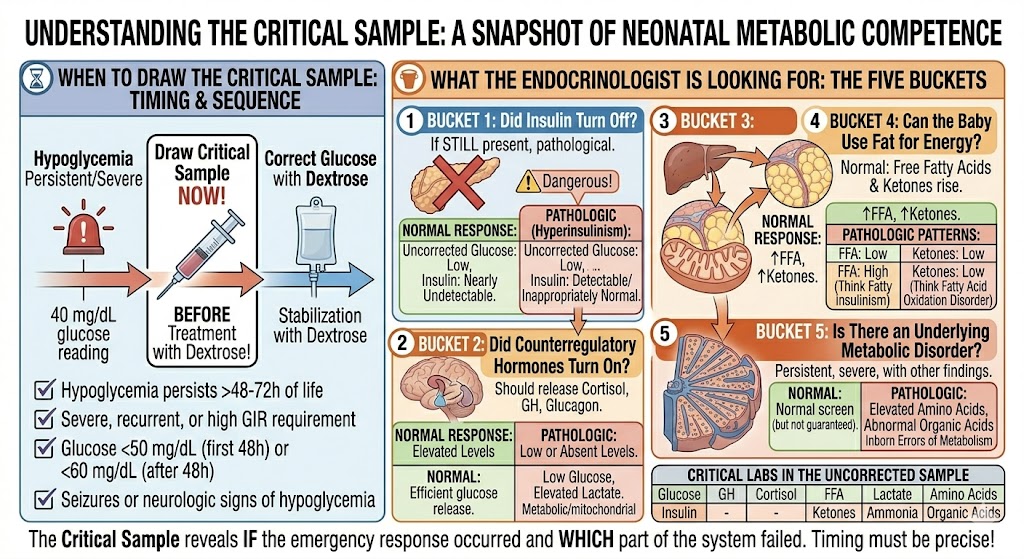
What the endocrinologist is looking for
Once the sample is drawn, the endocrinologist is working through five questions. Every lab in that critical sample fits into one of these buckets.
Question 1: Did insulin turn off?
When glucose falls, insulin should be nearly undetectable. If it's still present (even at levels that would seem normal in a fed state) it's pathologic in the context of hypoglycemia. Elevated or inappropriately detectable insulin tells the endocrinologist that hyperinsulinism is driving the picture.
What the labs show in hyperinsulinism:
Glucose: Low
Insulin: Detectable or inappropriately normal
Beta-hydroxybutyrate: Low
Free fatty acids: Low
In this scenario, insulin is simultaneously suppressing glucose production and shutting down access to stored fuel. The brain is getting neither glucose nor ketones. Exactly the dangerous pattern we discussed earlier.
Question 2: Did counterregulatory hormones turn on?
The body should be releasing cortisol, growth hormone, glucagon, and catecholamines in response to hypoglycemia. These hormones are trying to raise glucose. If they're low or absent during a hypoglycemic episode, the baby is unable to defend themselves. The cause may be hypopituitarism, growth hormone deficiency, or adrenal insufficiency.
Question 3: Can the liver make glucose?
If there's a problem with gluconeogenesis, glycogenolysis, or mitochondrial function, the liver can't produce glucose even when it's being told to. Elevated lactate can signal that the baby is relying on anaerobic metabolism or has an underlying metabolic pathway problem.
Question 4: Can the baby use fat for energy?
During hypoglycemia, a normal baby should be burning fat. Free fatty acids and ketones should rise. The pattern of what rises and what doesn't tells you a lot:
If neither fatty acids nor ketones rise → think hyperinsulinism
If fatty acids rise but ketones don't → think fatty acid oxidation disorder
This is one of the most clinically useful patterns in the critical sample because it helps distinguish between two very different problems that can look identical at the bedside.
Question 5: Is there an underlying metabolic disorder?
Now we're looking for less common causes: the inborn errors of metabolism that can present as persistent or recurrent hypoglycemia. A normal newborn screen does not rule these out. If hypoglycemia is persistent, severe, or accompanied by other findings like unusual odor, hepatomegaly, or neurologic symptoms, these labs become essential pieces of the puzzle.
What About Hyperglycemia?
NICU nurses spend a lot of time thinking about low glucose values, but high glucose values deserve just as much attention. And understanding hyperglycemia in the NICU requires letting go of how we think about high blood sugar everywhere else.
In older patients, hyperglycemia usually means too much glucose coming in, or insufficient insulin to handle it. In the NICU, especially in extremely preterm infants, it's a completely different problem. It's not primarily about intake. It's about an immature system that cannot regulate what's already there.
Here's what's happening physiologically: Stress hormones like cortisol and catecholamines actively drive gluconeogenesis and glycogenolysis, even when the baby is already receiving IV dextrose. The liver keeps producing glucose because the stress response is telling it to, regardless of what's coming in through the line. At the same time, relative insulin deficiency means the signal to stop producing glucose never arrives clearly. Extremely preterm infants also have reduced peripheral glucose uptake, so even available insulin isn't moving glucose into cells efficiently.
The result is a baby whose glucose keeps climbing despite your best efforts to reduce the GIR.
Contributing factors include:
Stress responses and illness severity
Excess glucose administration
Corticosteroid therapy
Catecholamine exposure
Relative insulin deficiency in extremely preterm infants
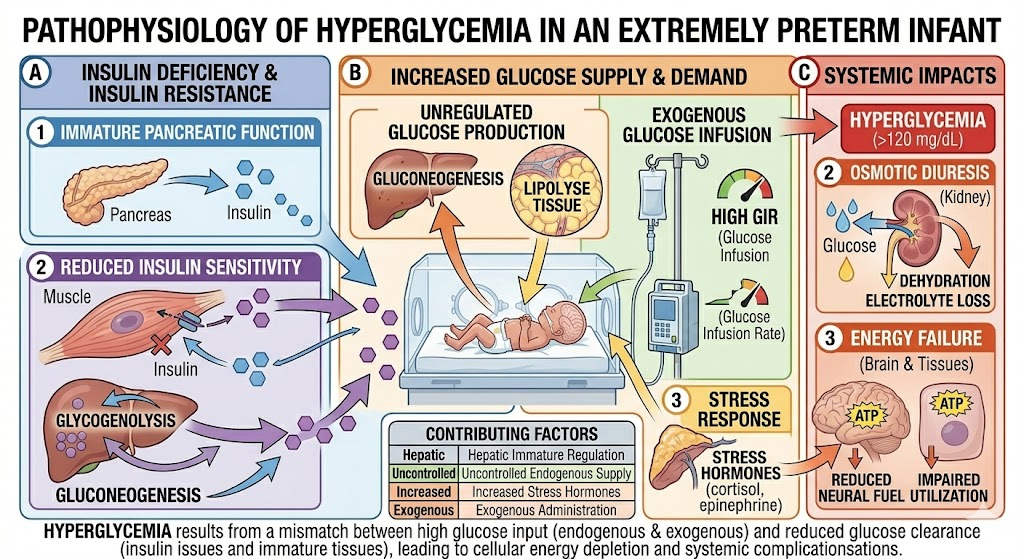
Why hyperglycemia matters
Hyperglycemia carries real clinical consequences. In extremely preterm infants, persistent hyperglycemia has been associated with increased risk of intraventricular hemorrhage, retinopathy of prematurity, increased susceptibility to infection, and higher mortality. The osmotic effects of high serum glucose draw fluid across cell membranes, which is particularly harmful to fragile, developing brain tissue.
When and How to Treat
This is where it gets nuanced, and where bedside nurses feel the tension most. There's no universal threshold that triggers treatment, and the evidence base for exactly when to intervene is still evolving. In general, when reducing the GIR to the lowest amount that still meets caloric needs doesn't resolve hyperglycemia, insulin infusions become the next tool.
But insulin in an extremely preterm infant is not without risk. The therapeutic window is narrow. Hypoglycemia from overtreatment can happen quickly, and the same vulnerabilities that made this baby hyperglycemic also make them susceptible to rapid glucose drops.
One more layer of complexity that doesn't always make it into the literature but matters enormously at the bedside: insulin adsorption.
Clinical Pearl: Insulin adheres to standard polyvinyl chloride (PVC) IV tubing. Depending on the tubing length and flow rate, a significant amount of the insulin you're infusing never actually reaches the patient. It's coating the inside of the line! This means the dose being delivered can be substantially lower than the dose that was ordered, especially at the low infusion rates used in the NICU.
Most NICUs address this with a tubing priming protocol: running insulin through the line for a set period of time before connecting it to the patient, allowing the binding sites in the tubing to saturate. Once the tubing is primed, insulin delivery becomes more predictable. But if that step is skipped or inconsistently done, you may spend hours wondering why the glucose isn't responding.
This is worth a direct conversation with your pharmacy. Priming protocols vary by institution, and some pharmacies prepare insulin syringes with priming built into the process. Knowing what your unit's protocol is (and why it exists) helps you troubleshoot when things aren't going as expected.
Some NICUs have also moved to low-sorbing tubing, sometimes called low-sorb tubing, which is specifically designed to minimize insulin adsorption. If your unit uses it, the priming concern is largely eliminated. If your unit doesn't, it's worth knowing that the option exists and advocating for it if insulin management is a recurring challenge in your population.
The practical takeaway: if an insulin infusion doesn't seem to be working, before assuming the dose needs to go up, ask whether the tubing was primed, how long the line has been running, and whether your unit has access to low-sorb alternatives. These small variables can make a significant difference in a population where glucose swings in either direction carry real consequences.
What Nurses Should Remember at the Bedside
When a glucose value is abnormal, don't stop at the number.
Ask yourself:
Why is this baby struggling to maintain glucose homeostasis?
Consider:
Is insulin too high?
Are energy stores too low?
Is glucose utilization increased?
Is glucose production impaired?
Does this baby have access to ketones as a backup fuel source? Or is that pathway suppressed too?
The answer helps guide both your assessment and your anticipation of the medical team's plan.
Imagine you're caring for a 28-weeker on day two of life whose glucose keeps trending up despite backing off the GIR. You could chase the number, or you could recognize the underlying physiology: immature counter-regulatory systems, stress hormones driving endogenous glucose production, relative insulin deficiency. That understanding changes how you communicate with the team and what you watch for next.
The best NICU nurses don't just recognize abnormal glucose values. They understand the physiology driving them.
High-Yield Certification Tip
When studying for the RNC-NIC or CCRN-N exams, focus less on memorizing lists and more on understanding the underlying physiology.
Most hypoglycemia questions can be answered by asking:
Is the baby making too much insulin, lacking energy stores, consuming glucose too quickly, or unable to produce enough glucose?
And for hyperinsulinemic hypoglycemia specifically remember that the danger isn't just the glucose. It's the simultaneous suppression of ketones, leaving the brain without any fuel source at all. Once you understand that framework, the risk factors and treatment strategies become much easier to remember.
Final Thought
Every newborn must make an incredible metabolic transition after birth. One that happens in seconds and unfolds over hours, with remarkably little margin for error.
For most infants, it happens seamlessly. For others, hypoglycemia or hyperglycemia is the first clue that something isn't adapting as expected.
The RNC-NIC and CCRN-N aren't testing whether you know that IDMs are at risk for hypoglycemia. They’re testing whether you understand the physiology well enough to predict what happens next. When you understand the physiology, the answers become easier because you're reasoning through the question rather than relying on memorization.
Ready to learn more neonatal physiology?
Glucose homeostasis is only one small piece of neonatal physiology. The same physiologic thinking applies to shock, endocrine disorders, congenital heart disease, ventilation, blood gases, and dozens of other concepts tested on the RNC-NIC and CCRN-N exams.
Stop wasting time memorizing lists that you'll forget by the end of your next 12-hour shift. Get the framework that makes physiology 'click' and walk into your exam knowing the why—so you can pass with confidence and provide better care at the bedside.
References
American Academy of Pediatrics, Committee on Fetus and Newborn, & Adamkin, D. H. (2011). Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics, 127(3), 575–579. https://doi.org/10.1542/peds.2010-3851
Karlsen, K. A. (2024). The S.T.A.B.L.E. program: Post-resuscitation/pre-transport stabilization care of sick infants: Guidelines for neonatal healthcare providers (7th ed.). S.T.A.B.L.E. Program.
McKinlay, C. J. D., Alsweiler, J. M., Ansell, J. M., Anstice, N. S., Chase, J. G., Gamble, G. D., Harris, D. L., Jacobs, R. J., Jiang, Y., Paudel, N., Signal, M., Thompson, B., Wouldes, T. A., Yu, T. Y., & Harding, J. E. (2015). Neonatal glycemia and neurodevelopmental outcomes at 2 years. New England Journal of Medicine, 373(16), 1507–1518. https://doi.org/10.1056/NEJMoa1504909
McKinlay, C. J. D., Alsweiler, J. M., Ansell, J. M., Anstice, N. S., Chase, J. G., Gamble, G. D., Harris, D. L., Jacobs, R. J., Jiang, Y., Paudel, N., Signal, M., Thompson, B., Wouldes, T. A., Yu, T. Y., & Harding, J. E. (2017). Association of neonatal glycemia with neurodevelopmental outcomes at 4.5 years. JAMA Pediatrics, 171(10), 972–983. https://doi.org/10.1001/jamapediatrics.2017.1579
Kau, S., Kahoano, L., Crowder, L., & Kenner, C. (2025). Metabolic system. In C. Kenner & J. Wright Lott (Eds.), Comprehensive neonatal nursing care (7th ed., pp. 209–229). Springer Publishing Company.
Stanley, C. A., Rozance, P. J., Thornton, P. S., De Leon, D. D., Harris, D., Haymond, M. W., Hussain, K., Levitsky, L. L., Murad, M. H., Simmons, R. A., Sperling, M. A., Weinstein, D. A., White, N. H., & Wolfsdorf, J. I. (2015). Re-evaluating "transitional neonatal hypoglycemia": Mechanism and implications for management. Journal of Pediatrics, 166(6), 1520–1525. https://doi.org/10.1016/j.jpeds.2015.02.045
Thornton, P. S., Stanley, C. A., De Leon, D. D., Harris, D., Haymond, M. W., Hussain, K., Levitsky, L. L., Murad, M. H., Simmons, R. A., Sperling, M. A., Weinstein, D. A., White, N. H., & Wolfsdorf, J. I. (2015). Recommendations from the Pediatric Endocrine Society for evaluation and management of persistent hypoglycemia in neonates, infants, and children. Journal of Pediatrics, 167(2), 238–245. https://doi.org/10.1016/j.jpeds.2015.03.057
Werny, D., Huang, A., Tenney, J., & Pihoker, C. (2024). Neonatal hypoglycemia and hyperglycemia. In R. J. Martin, A. A. Fanaroff, & M. C. Walsh (Eds.), Fanaroff and Martin's neonatal-perinatal medicine (12th ed., pp. 1254–1268). Elsevier.

Subscribe to my Mailing List
Get simple explanations of complex NICU topics, certification study tips, and practical bedside insights delivered straight to your inbox.
hey nurses don't miss out
© Copyright 2024. AmandasNICUEd. All rights reserved. | Terms & Conditions | Privacy Policy Contact: [email protected]