
Let's Keep in Touch
Follow me on Instagram or Facebook

Blogs & Articles
NEC Awareness
May 17 is NEC Awareness Day!
I will never forget one of my long-term primary patients from years ago—a preterm, growth-restricted baby boy. He was progressing steadily in the NICU until, seemingly overnight, everything changed. He was diagnosed with Stage III necrotizing enterocolitis (NEC) and underwent bowel resection, leading to short bowel syndrome (SBS). He needed a Broviac central line and was dependent on cyclic parenteral nutrition (PN) for growth.
Despite these challenges, he remained the sweetest soul, and his parents were resilient and devoted. They sent me Christmas cards for years after his discharge. Against the odds, he continued to grow and thrive, embodying both the devastation and hope wrapped in an NEC diagnosis.
This experience taught me that behind every NEC statistic is a child and family whose lives are forever altered. The month of May is NEC Awareness Month, and I'm reminded of why our vigilance and advocacy around this disease are so crucial.

⚠️ Necrotizing Enterocolitis
Necrotizing enterocolitis (NEC) is a devastating gastrointestinal disease that primarily affects our most vulnerable patients. The disease involves acute inflammation, bacterial invasion, and necrosis of the intestinal wall.
While most commonly seen in premature infants, particularly those born at less than 32 weeks gestation or with birth weights under 1500 grams, NEC also occurs in term neonates with predisposing conditions such as congenital heart disease or perinatal asphyxia.
NEC is not a singular disease but rather a spectrum of acquired intestinal injuries. This spectrum includes:
Classic NEC: The most common form, typically seen in preterm infants after the initiation of enteral feeds
Cardiac-induced NEC: Related to mesenteric hypoperfusion in infants with congenital heart disease
Atypical or transfusion-associated NEC: Often occurring within 48-72 hours of packed red blood cell transfusion
Term infant NEC: Usually associated with specific risk factors such as hypoxic-ischemic injury or polycythemia
Understanding these subtypes is essential for tailoring prevention strategies and treatment approaches to individual patients.
🌪️The Perfect Storm: Pathophysiology of NEC
NEC's pathophysiology is multifactorial, representing a "perfect storm" of conditions that converge in the vulnerable preterm gut. The key contributing factors include:
1. Prematurity and Intestinal Immaturity
The preterm infant's intestinal tract is characterized by:
Reduced barrier function with increased permeability
Immature tight junctions between enterocytes
Underdeveloped mucosal protective mechanisms
Insufficient production of protective antimicrobial peptides
Immature peristaltic patterns that prolong bacterial exposure
These factors create an environment where the intestinal barrier is easily breached, allowing bacterial translocation and triggering the inflammatory cascade.
2. Microbial Dysbiosis
The preterm infant's gut microbiome differs significantly from that of term infants:
Delayed colonization with beneficial bacteria
Dominance of potentially pathogenic species
Reduced microbial diversity
Higher concentrations of Proteobacteria (including Enterobacteriaceae)
Lower concentrations of Bifidobacteria and Lactobacilli
This dysbiosis is exacerbated by common NICU interventions such as antibiotic exposure, delayed feeding, and limited exposure to maternal microbiota.
3. Enteral Feeding Considerations
Feeding practices significantly impact NEC risk:
Breast milk reduces the risk of NEC risk 6-10 fold compared to formula feeding
Rapid advancement of feeds may overwhelm the immature gut
Hyperosmolar formulas and medications may damage intestinal mucosa
Human milk is protective through multiple mechanisms:
Immunoglobulins (particularly secretory IgA)
Lactoferrin with antimicrobial properties
Human milk oligosaccharides (HMOs) that promote beneficial bacteria
Growth factors that enhance intestinal maturation
Anti-inflammatory cytokines that modulate immune response
4. Immune Dysregulation
The preterm infant's immune system is characterized by:
Exaggerated pro-inflammatory responses
Ineffective regulation of inflammatory cascades
Overproduction of pro-inflammatory cytokines (TNF-α, IL-1β, IL-6, IL-8)
Increased toll-like receptor 4 (TLR4) expression, which recognizes bacterial lipopolysaccharide
Reduced production of anti-inflammatory mediators
This immune dysregulation creates a hyperinflammatory environment that contributes to tissue damage.
5. Impaired Intestinal Perfusion
Circulatory factors that contribute to NEC include:
Hypoxic-ischemic events that compromise intestinal blood flow
Hypotension requiring vasopressor support
Ductal steal phenomenon in infants with patent ductus arteriosus
Reduced microvascular density in the preterm intestine
Impaired autoregulation of mesenteric blood flow
Together, these factors result in a cycle of intestinal injury, inflammation, and progressive tissue damage that characterizes NEC.
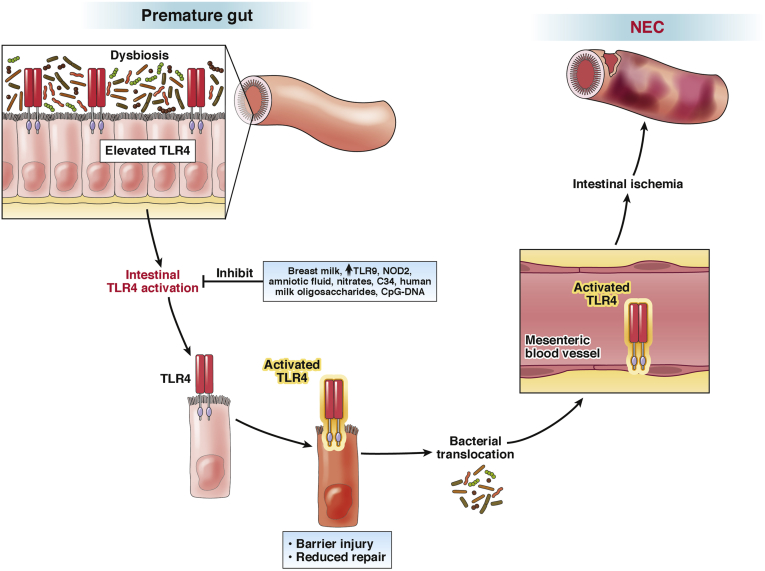
(Hackham & Sodhi, 2018)
🚨The Clinical Presentation: Recognizing NEC Early
Early recognition of NEC is critical for timely intervention. The clinical presentation typically includes a constellation of gastrointestinal and systemic signs.
Gastrointestinal Signs
Abdominal distention: Often one of the earliest signs, with progressive worsening
Bloody stools: Ranging from occult blood to grossly bloody diarrhea
Abdominal wall discoloration: Erythema or a bluish discoloration suggesting possible perforation
Palpable bowel loops: Indicating dilated, thickened intestinal segments
Decreased or absent bowel sounds: Suggesting ileus
Systemic Signs
Lethargy, apnea, bradycardia: Reflecting systemic involvement
Temperature instability: Often manifesting as hypothermia
Hypotension and poor perfusion: Indicating septic shock in advanced cases
Metabolic acidosis: Resulting from poor perfusion and anaerobic metabolism
Thrombocytopenia: A common hematologic finding that may precede other signs
Neutropenia or leukocytosis: Reflecting the inflammatory response
Radiologic Findings
Abdominal radiographs remain the cornerstone of NEC diagnosis:
Pneumatosis intestinalis: The radiographic hallmark of NEC, representing gas within the intestinal wall
Portal venous gas: Indicating more severe disease with bacterial translocation
Fixed, dilated intestinal loops: Suggesting areas of affected bowel
Pneumoperitoneum: Representing intestinal perforation, a surgical emergency
Early stages of NEC may show only nonspecific findings such as dilated bowel loops or a gasless abdomen, highlighting the importance of serial examinations and radiographs in suspected cases.
📊Staging Systems: Guiding Management Decisions
The modified Bell's staging criteria remain widely used to classify NEC severity and guide management:
Stage I: Suspected NEC
Mild systemic illness
Nonspecific gastrointestinal signs
Normal or nonspecific radiographic findings
Managed with antibiotics and bowel rest
Stage II: Definite NEC
Moderate systemic illness
Definite gastrointestinal signs
Pneumatosis intestinalis or portal venous gas on imaging
Managed with antibiotics, bowel rest, and supportive care
Stage III: Advanced NEC
Severe systemic illness with cardiovascular and respiratory compromise
Marked gastrointestinal signs with peritonitis
Pneumoperitoneum or other signs of perforation
Requires surgical intervention
Other classification systems incorporate laboratory values, such as thrombocytopenia and neutropenia, which are associated with poorer outcomes and may help identify infants requiring more aggressive intervention.

(Soni et al, 2020)
Arrow 1 shows the branching tree of the portal venous gas. Arrow 2 shows the crescents of pneumatosis. Arrow 3 shows widespread soap bubbling
🍼Prevention: The Best Treatment
Prevention remains the cornerstone of NEC management. Evidence-based strategies include:
Human Milk as Medicine
Mother's own milk (MOM) is optimal, with a dose-dependent reduction in NEC risk
Donor human milk (DHM) is preferable to formula when MOM is unavailable
Human milk-derived fortifiers may offer advantages over bovine-derived products
Human milk oligosaccharides (HMOs) promote a healthy microbiome and enhance gut maturation
Colostrum oral care (aka Oral Immune Therapy) provides local immune benefits even before enteral feeding is initiated
Standardized Feeding Protocols
Evidence-based advancement guidelines reduce practice variation
Slow advancement rates (15-20 mL/kg/day) may be safer for extremely preterm infants
Trophic feeding protocols that maintain gut stimulation shortly after birth
Careful monitoring parameters for signs of feeding intolerance
Standardized responses to feeding intolerance that avoid unnecessary withholding of feeds
Microbiome Protection Strategies
Avoiding unnecessary antibiotics preserves microbial diversity
Limiting duration of empiric antibiotics when cultures remain negative
Early skin-to-skin care promotes healthy microbial colonization
Avoiding H2 blockers and proton pump inhibitors that alter gut pH and microbial composition
Human milk feeding practices that support a healthy microbiome
Antibiotic Stewardship
Discontinuing antibiotics at 36-48-hours when cultures are negative
Narrowing antibiotic coverage based on culture results
Avoiding broad-spectrum antibiotics when narrower options are appropriate
Regular antibiotic timeout discussions among the healthcare team
Tracking antibiotic usage rates to identify opportunities for improvement
Probiotic Supplementation
Meta-analyses support probiotic efficacy in reducing NEC incidence
Multi-strain preparations may be more effective than single strains
Bifidobacterium and Lactobacillus species are most commonly studied
Safety considerations include risk of translocation sepsis in extremely preterm infants
There is currently no probiotic approved by the FDA to prevent NEC in preterm infants in the United States
Other Promising Approaches
Lactoferrin supplementation shows potential for NEC prevention
Pentoxifylline may modulate inflammatory responses
Stem cell therapies are being investigated for intestinal repair
Amniotic fluid components may promote intestinal development
Toll-like receptor modulators could prevent excessive inflammation
👩🏻⚕️When Prevention Fails: Treatment Approaches
Despite prevention efforts, NEC still occurs. Treatment approaches include:
Medical Management
Bowel rest: Withholding enteral feeds while maintaining nutrition via parenteral routes
Broad-spectrum antibiotics: Typically covering gram-negative, gram-positive, and anaerobic organisms
Gastric decompression: Reducing intestinal distention and bacterial proliferation
Fluid resuscitation and cardiovascular support: Maintaining adequate tissue perfusion
Correction of coagulopathy and thrombocytopenia: Reducing bleeding risk
Serial abdominal examinations and radiographs: Monitoring disease progression
Surgical Intervention
Approximately 30-50% of infants with NEC require surgical management. Indications include:
Pneumoperitoneum: Indicating intestinal perforation
Clinical deterioration despite maximal medical therapy
Abdominal wall erythema or discoloration
Surgical approaches include:
Primary peritoneal drainage: Often used as a temporizing measure in extremely preterm infants
Laparotomy with resection: Removing necrotic bowel segments
Creation of ostomies: Diverting intestinal contents
Long-term Outcomes and Complications
NEC survivors face significant short and long-term challenges:
Gastrointestinal Complications
Short bowel syndrome (SBS): Resulting from extensive intestinal resection
Intestinal strictures: Occurring in up to 35% of medically managed cases
Malabsorption and failure to thrive: Due to reduced absorptive surface area
Recurrent feeding intolerance: Requiring modified feeding approaches
Cholestatic liver disease: Associated with prolonged parenteral nutrition
Neurodevelopmental Outcomes
NEC survivors, particularly those requiring surgery, have higher rates of:
Cerebral palsy
Cognitive impairment
Hearing and visual impairments
Language delays
Behavioral challenges
These neurodevelopmental impacts may be related to inflammatory mediators affecting the developing brain, prolonged hospitalization, nutritional deficits, and associated comorbidities.
Family Impact
The impact of NEC extends beyond the infant to affect the entire family:
Prolonged hospitalization disrupting parent-infant bonding
Financial strain from medical expenses and lost work time
Emotional trauma associated with critical illness
Medically complex children with long-term complications
Increased parental stress and anxiety
Supporting NEC Survivors: The Long Road Ahead
Care for NEC survivors requires a multidisciplinary approach:
Nutritional Support
Specialized feeding approaches for children with short bowel syndrome
Monitoring for micronutrient deficiencies
Growth tracking with adjusted expectations
Transitioning from parenteral to enteral nutrition
Managing oral aversion and feeding difficulties
Developmental Follow-up
Early intervention services
Regular developmental assessments
Specialized therapies (physical, occupational, speech)
Educational support and advocacy
Family support resources
Building Resilience
Despite the challenges, many NEC survivors demonstrate remarkable resilience. Supporting this resilience involves:
Celebrating small victories
Building support networks
Connecting with other NEC families
Focusing on capabilities rather than limitations
Advocating for needed services and resources

NEC Awareness and Advocacy: Making a Difference
May 17th is designated as NEC Awareness Day, providing an opportunity to:
Educate healthcare providers about prevention strategies
Raise public awareness about this devastating disease
Support research initiatives seeking better prevention and treatment
Connect families affected by NEC with resources and support
Advocate for policies that support human milk feeding and optimal NICU care
Organizations like the NEC Society bring together researchers, clinicians, and families to advance prevention, treatment, and support for those affected by NEC.
NEC remains one of the most challenging diseases in neonatal care, but there is reason for hope. Advances in understanding the pathophysiology, improving prevention strategies, and developing targeted therapies offer promise for reducing the burden of this disease.
As NICU nurses, our vigilance in identifying early signs, our advocacy for evidence-based prevention practices, and our compassionate care for affected infants and families make a profound difference. Every baby spared from NEC represents a family saved from trauma and a life preserved from potential long-term complications.
During NEC Awareness Month, let us commit to continued progress toward a future where NEC no longer devastates our most fragile patients.
Resources for Families and Professionals

Let's work together to create a world without NEC.
Wishing you the best
Amanda
References
Keefe G, Jaksic T, Neu J. Necrotizing Enterocolitis and Short Bowel Syndrome. In: Martin RJ, et al. Fanaroff and Martin's Neonatal-Perinatal Medicine. 11th ed. 2020
de la Cruz D, Gipson DR. Moving Beyond NEC. In: Martin RJ, et al. Fanaroff and Martin's. 11th ed. 2020
Ortigoza EB. Feeding Intolerance. In: Kliegman R, et al. Nelson Textbook of Pediatrics, 21st ed. 2020
National Association of Neonatal Nurses. Neonatal Parenteral and Enteral Nutrition: A Resource Guide for the Student and Novice Neonatal Nurse Practitioner. 2020
Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. 2011;364(3):255–264. doi:10.1056/NEJMra1005408
Sharif S, et al. Probiotics to prevent NEC in very preterm or very low birth weight infants. Cochrane Database Syst Rev. 2020;10:CD005496. doi:10.1002/14651858.CD005496.pub5
Gephart SM, McGrath JM. NEC Zero: A prevention-focused approach. Adv Neonatal Care. 2012;12(1):23–32. doi:10.1097/ANC.0b013e3182425df0
Hackam DJ, Sodhi CP. Toll-like receptor-mediated intestinal inflammatory imbalance in the pathogenesis of necrotizing enterocolitis. Cell Mol Gastroenterol Hepatol. 2018;6(2):229-238.e1. doi:10.1016/j.jcmgh.2018.04.001
Hair AB, et al. Beyond necrotizing enterocolitis prevention: Improving outcomes with an exclusive human milk-based diet. Breastfeed Med. 2016;11(2):70-74. doi:10.1089/bfm.2015.0134
Patel RM, Denning PW. Intestinal microbiome and its relationship with necrotizing enterocolitis. Pediatr Res. 2015;78(3):232-238. doi:10.1038/pr.2015.97
How to use abdominal X-rays in preterm infants suspected of developing necrotising enterocolitis. Archives of Disease in Childhood - Education and Practice 2020;105:50-57.
Missed my other newsletters? Click here to read them!
Let's Study Together! Join my Certification Course


hey nurses don't miss out
© Copyright 2024. AmandasNICUEd. All rights reserved. | Terms & Conditions | Privacy Policy Contact: [email protected]